Interview with Marisa Padgett, LCSW, conducted by Alex Levitt
“These kids are trying to live a life that is authentic to what is going on inside of them, and when loved ones reject them, that is detrimental to the kid’s mental health and self-esteem.”
In what ways do you see changes when it comes to acceptance of LGBTQ+ youth in society?
Marisa Padgett: It’s interesting because I recently talked to a 12-year-old boy here who identified as gay. I was speaking with the grandmother, and she was worried at how society at large will accept him. While she accepts him, she has her fears. We were talking about how acceptance has changed a lot in the last 10 to 20 years. I remember that when I was in high school, most people were not out. It was getting more accepted, but not how it is now.
I don’t worry as much about the kids with their peers, but more when they are out in the community. I think it has gotten better, but there is still a long way to go. In some ways, now it is more divisive than ever. I think that people are very hard-lined where they stand, either one way or another. While the LGBTQ+ community is growing, and we have things in place for pride and a lot of support for the kids in this community, there are people out there who are rejecting and intolerant, and they skew toward hate just for hate’s sake.
Middle school kids can also be very vocal and put down kids for any reason because that’s kind of where they are in life, developmentally. Also, generational issues surface a lot – for example, “My mom gets me, but she says don’t tell my grandparents that I’m transgender.” There is still a lag generationally. There can also be a shift in a relationship between a kid and loved ones after coming out. When the reality of it hits the parents, some have a hard time reconciling this new information about their kid’s identity.
How can we build an atmosphere of inclusion, regardless of our personal or religious views?
MP: We tell families that when a child comes out, this is who they are; they are not different people. What you think about a person before you found out they are gay, transgender or non-binary is still true because they are still that same person. There are many layers to people. Recognizing this is important for the families and for the society at large in becoming more tolerant. Look at people as people who are living their lives and their identity, and recognize it is not something they are choosing. We try to help parents understand they are not choosing this because in truth, it is a hard path. Having to deal with the prejudice, intolerance and the outright hate out there is immensely difficult.
Asking yourself what if it was your child, sister, brother or parent is a helpful exercise. If it was someone that you love deeply, would that be any different for you? Also, if an LGBTQ+ youth is not accepted by their peers, maybe they need to hang out with different people. A club like GSA [Gay-Straight Alliance] has done wonders for giving young people a space of acceptance. Everyone is entitled to their beliefs, absolutely, but that should not affect how other people should be treated in society.
What are the mental health challenges facing LGBTQ+ youth, and how can loved ones can be supportive?
MP: We are seeing a lot of young people dealing with depression, anxiety, suicidal thoughts and self-harm. I think it is a result of the fear of not being accepted and the way that the people closest to them will respond. It’s a very different thing if they are not openly LGBTQ+, but they almost know that their parents will not accept them. They’ve heard the way their parents talk about it, or for instance say their cousin came out and they heard their parents’ talk negatively about it. These kids are aware and have an idea already of how their parents are going to react. They might be out to their friends, but having to hold that in and not being comfortable with who they are in front of their parents causes a lot of tension.
Coming out must be handled very sensitively. Parents need to figure out how to respond to their teen, especially if they are already depressed or having suicidal thoughts. An issue with those who identify as transgender and non-binary is they have come out and the parents won’t accept them or use their pronouns. I tell the kids that if their parents are trying that’s good, but when parents refuse, that’s where the friction happens, and the kids struggle with mental health issues. These young people are trying to live a life that is authentic to what is going on inside of them, and when loved ones reject them, that is detrimental to the kid’s mental health and self-esteem. It’s like saying, “It’s not okay to be who you are”. Kids can attempt to take their lives over this.
What services does North Shore Child & Family Guidance Center provide LGBTQ+ youth to help them?
MP: There are basic services we provide like individual and family therapy. We build an LGBTQ+ group every fall once we have enough clients. Every therapist here is understanding and aware of LGBTQ+ issues. As a supervisor, I educate my team and make sure they are all very aware and sensitive and supportive. We do the family work and help the parents with the issues that they themselves are struggling to accept and understand for the child.
During the intake process, we ask the child in private if they want to address their sexual orientation or identity in treatment. In addition, we ask if their parents know and if they want them to know. You don’t want to assume anything. Making them comfortable to open up is vital to treatment.
Bio: Marisa Padgett, LCSW, is Clinical Supervisor of Emergency, Triage & Suicide Prevention Services at North Shore Child & Family Guidance Center. She can be reached at mpadgett@northshorechildguidance.org or 516-626-1971, ext. 367.
Bio: Alex Levitt is a senior at Farmingdale State College, where he is majoring in Professional Communications. He is an intern for North Shore Child & Family Guidance Center, Long Island’s preeminent children’s mental health organization. To reach the Guidance Center, call 516-626-1971.
Research on LGBTQ+ Youth
LGBTQ+ identified individuals have a 2 to 6 times higher lifetime risk of suicide and/or depression than the general population.
The concept of “dual alienation” is the idea that individuals who belong to more than one marginalized group are doubly marginalized. Individuals with mental health issues who identify as LGBTQ belong to at least two traditionally marginalized groups.
Suicide is the second leading cause of death among young people aged 10 to 24— and lesbian, gay, bisexual, transgender, queer and questioning LGBTQ+ youth are at significantly increased risk.
The Trevor Project estimates that more than 1.8 million LGBTQ+ youth (13-24) seriously consider suicide each year in the U.S. — and at least one attempts suicide every 45 seconds.
The Trevor Project’s 2022 National Survey on LGBTQ+ Youth Mental Health found that 45% of LGBTQ+ youth seriously considered attempting suicide in the past year, including more than half of transgender and nonbinary youth.
The data show that 43% of transgender youth have been bullied on school property. 29% of transgender youth, 21% of gay and lesbian youth and 22% of bisexual youth have attempted suicide
16% of gay and lesbian youth and 11% of bisexual youth have been threatened or injured with a weapon on school property, compared to 7% of straight youth.
North Shore Child & Family Guidance Center is pleased to announce that Jennifer Rush has joined the organization as Associate Executive Director. Ms. Rush will be reporting to Executive Director/CEO Kathy Rivera.
Ms. Rush began her career at the Foundation for Childhood Development in NY as a research assistant, where she explored case studies of how systems support children to reach their full potential. She has a diverse operations background in medical, educational and community-based services, including hospital and substance abuse settings at Northern Berkshire Healthcare and the Brattleboro Retreat.
Most recently, Ms. Rush was the Vice President of Residential and Clinical Services at Berkshire County Arc in Pittsfield, Mass., where she oversaw all residential services, including the autism outreach services program and the brain injury services program. repeated “With more than 28 years of leadership experience in nonprofit, residential and health care settings, Jennifer has extensive experience working with adults, children and families in mental health and substance use,” said Kathy Rivera, Executive Director/CEO of the Guidance Center. “Her impressive level of knowledge, skill and expertise sets the stage for continued growth and expansion of the Guidance Center and will help strengthen our services across the agency.”
“I am excited to have returned to New York to work at the Guidance Center and find ways to further support the agency’s mission of bringing hope and healing to children and families,” said Ms. Rush. “I am also eager to support the Guidance Center’s incredibly dedicated employees who provide their clients g with compassionate, high-quality services that truly save lives.”
Ms. Rush, who holds a B.A. from Barnard College and a Master of Health Care Administration from Seton Hall University, moved from the Berkshires region of Massachusetts to Long Island’s North Shore in May 2022. “My two college-age children and our golden retriever are all making the transition,” she said, “and in a very short time, we are all already feeling at home.”
By guest blogger Alex Levitt, to be published in Anton Media July 1, 2022
I grew up as a sensitive kid. So much so that when my elementary school gave out superlatives to graduating 5th graders, the one I received was most self-aware. Growing up, I viewed my sensitivity as a weakness, a clear marker that separated me from my peers and gave high stakes to any social interaction I happened to find myself in. I didn’t really understand why I felt so different from other kids my age. Most seemed to wade through childhood keeping their head above water, impervious to insults and not getting bogged down in their own self-image.
Middle school is when I had my first depressive episode. It was the summer going into 8thgrade, and I got blindsided by a special brew of anxiety for the future and a persistent inner critic that wouldn’t give me any time to myself. Another wrinkle added to my situation was that my anxiety made me sick to my stomach so I could not keep down any food I ate.
This first dance in the waters of depression lasted about three weeks, which seems like the most minor of blips compared to the length of time I have been depressed since then. I have lost count of how many times depression has darkened my door. When my symptoms re-emerged, it was dispiriting because I convinced myself I was past it and would never “regress” in that way.
Yet, I don’t regret any of it. It has made me stronger, surer of myself, and—most importantly to me—compassionate about other’s hardships. Through the trial of adversity, I decided to choose growth. Not that this was easy. My biggest hurdle was bypassing my own stubbornness. I had to take my experiences and view them as a chance to better myself instead of beating myself up over my perceived “weakness.”
Mental health awareness and ending stigma is very important to me. Not just because of my own exposure, but because of the many friends and family members I have seen affected by various mental health issues. I continue to meet so many amazing and brilliant people who suffer internally because of something out of their control.
My experience and that of others made me curious about what mental health services were offered at my school, Farmingdale State College. I saw that there was one-on-one counseling on campus, but there was a lack of specialized services or peer support groups. In spring of 2021, I was part of the Student Government Association (SGA) at Farmingdale, and each semester a Senator is required to present his/her own resolution with the goal of improving services for students on campus.
I couldn’t think of a better idea than to center my resolution on expanding the mental health services on campus. There used to be more student resources for this, but the pandemic had limited those services and had yet to return in full force with options for the students. My resolution was aimed at addressing the addition of more support groups for students to discuss issues they were experiencing during the school year, and to cover a wider range of mental health concerns, such as social anxiety, depression, addiction and other mood disorders.
It got passed on the Senate floor, but it still took a while for the changes to be instituted. Luckily, a fellow Senator helped things progress further this past fall by adding his own resolution calling for more mental health services, which in effect expanded upon my resolution. This past spring, I saw flyers and even an electronic sign in front of campus advertising support groups for students, whether for anxiety, depression or other mental health issues.
There is always more to be done, but it is important that we fight to give those suffering a place where they feel they can be heard and that they are not alone.
Bio: Alex Levitt is a senior at Farmingdale State College, where he is majoring in Professional Communications. He is an intern for North Shore Child & Family Guidance Center, Long Island’s preeminent children’s mental health organization. To reach the Guidance Center, call 516-626-1971.
In 2021, North Shore Child & Family Guidance Center continued to respond to the mental health challenges among our youth, which the U.S. Surgeon General deemed a true crisis. While the pandemic exacerbated these challenges among children and teens, the rates of suicidal thinking, depression, anxiety and other issues have been on the rise for well over a decade.
In our Annual Report, we give you an overview of the year that was, including a rundown of our programs and services; success stories and letters from our families; and a special feature focusing on two of our most important programs: the Douglas S. Feldman Suicide Prevention Project and the Fay J. Lindner Foundation Triage and Emergency Services.
We could not provide these lifesaving services to the community without the support of all our treasured donors, including you.
Thank you for allowing us to bring hope and healing to the children and families of Long Island.
There may be no scarier words for a parent to hear from their child than “Some days I just don’t think I can go on any longer,” or a similar sentiment. The reality is that children and teens are under more stress than ever, with suicidal thinking and actions on the rise over the past decade. Moreover, the isolation and fear surrounding the pandemic has created a dramatic increase in severe depression and anxiety.
But even before COVID-19 upended our lives, North Shore Child & Family Guidance Center was responding to the crisis in suicidal thinking and actions among young people with two initiatives focused on saving lives: the Douglas S. Feldman Suicide Prevention Project and the Fay J. Lindner Foundation Triage and Emergency Services.
Answering the Call
In 2021, the Guidance Center experienced a substantial increase in referrals from schools, pediatricians, hospitals and others. Those entities know that we promise to see urgent cases within 24 to 48 hours—an unheard-of response time, when most families are faced with waits of weeks or even months to get help for their children.
In fact, recent stories in the New York Times and other sources report that suicidal children and teens often wait in emergency exam rooms for days or even weeks to access urgently needed treatment. Both inpatient and outpatient mental health services, even when a situation is clearly an emergency, are in extremely short supply.
By contrast, when an urgent call comes into the Guidance Center, our most senior triage clinicians and their team members assess each individual case, working collaboratively with the family and child to create a treatment plan that provides the care these vulnerable children and teens need to begin on the road to healing.
We address all high-risk cases with a thorough evaluation for suicide risk; multiple sessions of individual, group and family therapy each week for as long as is needed; and an individualized treatment plan that focuses on safety strategies and healthy coping skills.
A key element in the creation of a safety plan is a list of prioritized coping strategies and sources of support that children and teens can use during times of crisis. We have found that this is an essential process to help engage our high-risk clients during a most vulnerable time.
We also provide educational seminars, both in person and via webinars, on suicide prevention, so that parents, students, medical professionals and school administrators learn to recognize the signs and know what resources are available to them, including our services.
Treating the Whole Child
The Guidance Center team knows the importance of treating our clients with a holistic, expansive approach, so our clinicians work closely with the family, schools and other entities to explore whether the systems in place are a good fit for the child.
Some of our young clients have suffered with extreme bullying, academic failure, lack of support in their schools and other traumatic situations. To address all of a child’s emotional needs, we advocate for more support services, whether it means securing additional accommodations in the school, offering a different setting that is more therapeutic or providing case management for the family.
Our clinicians are a lifeline to kids and parents, providing emotional support, state-of-the-art clinical services, community resources and concrete steps that enable them to move beyond despair and hopelessness so they can envision a truly bright future.
Donors Make the Difference
Without the generosity of Ellen and Donald Feldman, who funded the program in honor of their son, and the trustees at the Fay J. Lindner Foundation, our lifesaving services would not be possible. To them, and all of you who donate to support the Guidance Center, we are profoundly grateful.
To learn how to support our work, contact Lauren McGowan, Director of Development, at LMcGowan@northshorechildguidance.org, or call 516-626-1971, ext. 320.
With inpatient psychiatric services in short supply, adolescents are spending days, even weeks, in hospital emergency departments awaiting the help they desperately need.
On a rainy Thursday evening last spring, a 15-year-old girl was rushed by her parents to the emergency department at Boston Children’s Hospital. She had marks on both wrists from self-harm and a recent suicide attempt, and earlier that day she confided to her pediatrician that she planned to try again.
At the E.R., a doctor examined her and explained to her parents that she was not safe to go home.
“But I need to be honest with you about what’s likely to unfold,” the doctor added. The best place for adolescents in distress was not a hospital but an inpatient treatment center, where individual and group therapy would be provided in a calmer, communal setting, to stabilize the teens and ease them back to real life. But there were no openings in any of the treatment centers in the region, the doctor said.
Indeed, 15 other adolescents — all in precarious mental condition — were already housed in the hospital’s emergency department, sleeping in exam rooms night after night, waiting for an opening. The average wait for a spot in a treatment program was 10 days.
The girl and her family resigned themselves to a stay in the emergency room while she waited. But nearly a month went by before an inpatient bed opened up.
The girl, being identified by her middle initial, G, to protect her privacy, spent the first week of her wait in a “psych-safe” room in the emergency department. Any equipment that might be used for harm had been removed. She was forbidden to use electronics — to keep her from searching the internet for ways to commit suicide or asking a friend to smuggle in a sharp object, as teens before her had done. Her door was kept open night and day so she could be monitored.
It was “padded, insane-asylum-like,” she recalled recently in an interview. “Just walls — all you see is walls.”
She grew “catatonic,” her mother recalled. “In this process of boarding we broke her worse than ever.”
G’s story describes one of its starkest manifestations of the crisis. Across the country, hospital emergency departments have become boarding wards for teenagers who pose too great a risk to themselves or others to go home. They have nowhere else to go; even as the crisis has intensified, the medical system has failed to keep up, and options for inpatient and intensive outpatient psychiatric treatment have eroded sharply.
Nationally, the number of residential treatment facilities for people under the age of 18 fell to 592 in 2020 from 848 in 2012, a 30 percent decline, according to the most recent federal government survey.The decline is partly a result of well-intentioned policy changes that did not foresee a surge in mental-health cases. Social-distancing rules and labor shortages during the pandemic have eliminated additional treatment centers and beds, experts say.
Absent that option, emergency rooms have taken up the slack. A recent study of 88 pediatric hospitals around the country found that 87 of them regularly board children and adolescents overnight in the E.R. On average, any given hospital saw four boarders per day, with an average stay of 48 hours.
“There is a pediatric pandemic of mental health boarding,” said Dr. JoAnna K. Leyenaar, a pediatrician at Dartmouth-Hitchcock Medical Center and the study’s lead author. In an interview, she extrapolated from her research and other data to estimate that at least 1,000 young people, and perhaps as many as 5,000, board each night in the nation’s 4,000 emergency departments.
“We have a national crisis,” Dr. Leyenaar said.
This trend runs far afoul of the recommended best practices established by the Joint Commission, a nonprofit organization that helps set national health care policy. According to the standard, adolescents who come to the E.R. for mental health reasons should stay there no longer than four hours, as an extended stay can risk patient safety, delay treatment and divert resources from other emergencies.
Yet in 2021, the average adolescent boarding in the E.R. at Boston Children’s Hospital spent nine days waiting for an inpatient bed, up from three and a half days in 2019; at Children’s Hospital Colorado in Aurora in 2021, the average wait was eight days, and at Connecticut Children’s Medical Center in Hartford, it was six.
Emergency-department boarding has risen at small, rural hospitals, too, with “no pediatric or mental health specialists,” said Dr. Christian Pulcini, a pediatrician in Vermont who has studiedthe trend in the state. “There is one clear conclusion,” he told the Vermont legislature recently. “The E.D. is not the appropriate setting for children to get comprehensive, acute mental health services.”
Doctors and hospital officials emphasize that adolescents should absolutely continue to come to the E.R. in a psychiatric emergency. Still, many emergency-room doctors and nurses, trained to treat broken bones, pneumonia and other corporeal challenges, said the ideal solution was more preventive care and community treatment programs.
“Frankly speaking, the E.D. is one of the worst places for a kid in mental health crisis to be,” said Dr. Kevin Carney, a pediatric emergency room doctor at Children’s Hospital Colorado. “I feel at a loss for how to help these kids.”
‘Actually a good day’
The challenge was evident one day in late February when Dr. Carney arrived for his shift at 3 p.m. The children’s hospital has 50 exam rooms in its emergency department, which fill with patients who have gone through an initial screening and need further evaluation. By midafternoon, 43 of the rooms were full, 17 of them with mental health cases.
“It’s breathtaking,” Dr. Carney said as he stood in the hallway. “Forty percent.”
On clocking in, Dr. Carney had inherited a block of 10 exam rooms from a doctor who was clocking out. “Seven are mental health issues,” Dr. Carney said. “Six are suicidal. Three of them made attempts.”
The adolescents who were deemed to be at physical risk to themselves or others could be readily identified: Their exam room doors were open so they could be monitored, and they wore maroon-colored scrubs instead of their own clothes. No shoelaces, belts or zippers.
Throughout the day, staff members at the hospital had called eight inpatient facilities in the region, looking for available slots in treatment centers where the 10 young boarders, as well as 17 other adolescents boarding at three smaller Colorado Children’s Hospital campuses around the state, could be placed.
One of the adolescents waiting in Aurora, a Denver suburb, was a 16-year-old who had been stabilized after attempting suicide and who needed a residential treatment spot. “But there are no beds,” Jessica Friedman, a social worker, said she had told the family.
“I have eight or nine conversations like this a day,” Ms. Friedman, standing in the hallway, told a reporter; so far that day she had had only two. “This is actually a good day.”
Standing nearby, Travis Justilian, a nurse and the interim clinic manager in the emergency department, said the flood of boarders “is crushing our staff.” He added, “We’re fixers and we’re sitting here doing nothing but watching them watch TV.”
Colorado is struggling with the same shortage of services that has hit hospitals nationwide. The state has lost 1,000 residential beds serving various adolescent populations since 2012, according to Heidi Baskfield, vice president of population health and advocacy for Children’s Hospital Colorado. The state closed one 500-bed facility, Ridgeview, which served at-risk young people, in 2021 because of instances of poor quality and abuse. Another facility, Excelsior, closed its 200 beds in 2017 because reimbursement rates were not high enough to support ongoing operations, the chief executive officer said at the time of the closing.
A major cause, Ms. Baskfield said, was the low reimbursement rates paid by Medicaid, the state insurance program. From 2006 to 2021, the daily Medicaid rate in Colorado allotted roughly $400 for a therapeutic residential bed — “less than some families spend to send their kids for a night to sleepaway camp,” Ms. Baskfield said.
The low rates also accounted for some of the quality issues, she said; it was hard to hire experienced staff. (In the past year, Colorado has raised its reimbursement to $750 per day by using money from the American Rescue Plan, but new beds have yet to open, and that source of money is temporary.)
Lisette Burton, chief policy and practice adviser for the Association of Children’s Residential and Community Services, a nonprofit advocacy group, noted that, nationally, the closure of facilities and the loss of beds was the result of many factors, including a well-intended, decades-long effort to keep foster children and other children out of institutional settings. But the intended substitutes — more nimble and specialized treatment options — were never funded and remain largely unavailable, she said.
Then came the pandemic, amplifying labor shortages and introducing social-distancing and quarantine guidelines that reduced the capacity for patients. “Demand went up, supply went down,” Ms. Burton said. “Now we’re in full-blown crisis.”
On that February day in Colorado, one inpatient bed finally opened up. It happened to be in the 12-bed inpatient ward of Children’s Hospital Colorado, just a few minutes’ walk from the E.R.
The ward’s hallways are wide, the walls painted light green and the lighting bright, to instill a feeling of comfort and calm. Each bedroom has windows looking outside and, next to the door, a glass panel enabling hospital staff to discreetly peer inside.
In a small communal room, four adolescent girls in maroon scrubs sat on blue chairs and couches. One listened to headphones and sang aloud to the soundtrack to “Encanto.” Another worked on a jigsaw puzzle of the sea. Two others chatted with a counselor.
The emergency department “is just a collection of rooms where patients are expected to stay in their rooms and comply with rules,” said Lyndsay Gaffey, director of patient care services at Children’s Hospital Colorado. In the inpatient ward, she said, the aim instead was to stabilize patients by having them work through trauma, receive therapy and interact with peers.
But they must be closely watched here, too. When a reporter rested a pen on a countertop, a staff member swept it up. “You cannot have this here unless it is on your person,” she said. “If a patient walks over and grabs it, it can basically be used as a weapon.”
How to Help Teens Struggling With Mental Health
Recognize the signs. Anxiety and depression are different issues but they do share some indicators. Look for changes in a youth’s behavior, such as disinterest in eating or altered sleep patterns. A teen in distress may express excessive worry, hopelessness or profound sadness.
Approach with sensitivity. If you are seeking to start a discussion with a teen who might be struggling, be clear and direct. Don’t shy from hard questions, but also approach the issue with compassion and not blame.
Get the correct diagnosis. Find the right doctor for your child by asking for recommendations. Ask the specialist about her experience treating specific conditions in children and the measurement tools she uses to make medical assessments.
Carefully consider medications. Press doctors on their experience treating children with specific drugs and make sure you understand their side effects and interactions with other treatments, as well as how to tell if a medication is working and how hard it is to wean off of it.
Don’t forget the basics. Young people, with developing brains, need eight to 10 hours of sleep to promote mental and physical health. Lack of sleep can interfere with development, and can dramatically impact mood. Physical activity is also vital.
Is it safe to go home?
In severe cases of mental distress, emergency-room doctors can compel an adolescent to board in the E.R. until inpatient services become available, however long that takes. Often, parents opt to return home with their child, to try to manage there while waiting for a treatment opening. But that option requires family and doctors alike to work through a difficult question: Is the adolescent safe to go home?
In early February, a 12-year-old boy, J, was struggling toward an answer at the emergency room of the Highlands Ranch campus of Children’s Hospital Colorado. (He is being identified by his first initial for privacy reasons.)
He had arrived that morning with his mother, after she discovered that he had been searching the internet for ways to commit suicide. Over the course of his day in the E.R., he was asked several times how safe he felt to go home. The mother recounted one exchange:
“Do you think you can go home?” the doctor asked.
“What’s the other option?” J asked.
“You’d be in the emergency room.”
“I can go home with my mom,” J said. “But if I feel like I’m going to kill myself, what do I do?’”
“You’ll come back to the emergency room,” the doctor replied.
J’s mother took him home and “hid every medicine and every knife,” she said. J wanted to get help and asked her that first night: “So can I start tomorrow?”
No, his mother told him, he’d have to wait. Sixteen days went by before a spot for J opened in an intensive treatment program. She watched her son around the clock. “It was the scariest two weeks of my life,” she said.
The longest wait
For adolescents like G, who stayed in the emergency room of Boston Children’s Hospital last spring, the experience can be wrenching.
G lives in a Boston suburb with a teenage brother, father and mother. The family has a history of anxiety and depression, the mother said, but G had been a happy and adventurous child. In middle school she started talking back and acting somewhat obsessively, behavior that her mother figured was typical for a teenager.
What G’s mother did not know was that her daughter had been cutting herself for two years, since seventh grade, before the pandemic began. “I cut with literally anything I could find — hockey cards, pipe cleaners, paper clips, anything,” G said. She described the self-harm as a “coping mechanism” to deal with inner pain. She hid the activity “with sweaters, hoodies, foundation.”
As the pandemic set in, G withdrew, and her grades fell. “Then came April 29,” her mother said. “We had a life before April 29 and a life after April 29.”
That day, she picked up G at school for a routine visit to the pediatrician. As G got into the car, her mother saw the marks on her wrists.
At the emergency room, G told the medical team she had tried to overdose a few weeks earlier and had regretted the next morning that she was still alive. In the exam room, she noticed a container of hand sanitizer. “I told them, ‘I’m thinking about drinking this,’” G recalled.
Admitting to her pain and self-harm provided her “with kind of a little bit of relief,” she said. “After two years of cutting and trying to kill myself, I was finally going to get some help. But I didn’t really get help.”
That first night, she was moved for safety reasons to a room that contained just a bed and, for her mother, a rollaway. With the door open, sleeping was difficult. “A sitter was literally staring at my kid,” G’s mother said. “It felt demoralizing.”
Mother and daughter played Uno, Go Fish, checkers and Connect Four. G, anxious and awake, received Ativan on three of the next four nights, then was prescribed Trazodone for chronic anxiety.
Boarding night after night in an emergency department can overwhelm some adolescents, said Dr. Amanda Stewart, an emergency room pediatrician at Boston Children’s. One day this February, she was treating an infant with a respiratory infection when she heard screaming. It came from a 12-year-old boy with attention-deficit disorder and autism who had threatened suicide and was boarding down the hall.
“Other patients started escalating,” Dr. Stewart recalled. “One of them, across the hall, started hitting her head against the wall.” The girl, 15, had entered the E.R. after a suicide attempt and had been calm until that point.
Dr. Stewart said that some teens tell her that boarding in the emergency department intensified their suicidal urges. “I’ve heard that from kids many times,” she said, recalling that they will say: “‘I’m not going to tell you next time, because it means I’m going to have to come here again.’”
Dr. Patricia Ibeziako, a child psychiatrist at Boston Children’s Hospital, said that adolescents do, in fact, receive some treatment while boarding in the emergency department, including basic counsel aimed at “crisis stabilization” that is “all geared to safety.”
“Boarding is not a great thing, but it’s still care,” Dr. Ibeziako said. “We’re not just putting a kid in a bed.”
Kid on fire
May 7 arrived — G’s eighth day in the emergency ward — and still no inpatient beds were available in the region. But a bed did open in the hospital, upstairs in the pediatric medical unit; this room had a window and a private bathroom, and a caregiver who watched G around the clock.
She “was very, very, very depressed and dejected,” her mother recalled. “She didn’t even cry anymore.”
Finally, 29 days after G arrived, a bed was located for her at an inpatient facility in an outlying suburb. She spent a week there but did not find the experience all that helpful.
“We learned the same coping skills over and over,” she said. Over the summer, she worked a fast-food job, but she continued cutting herself, she said, and did a better job of hiding it.
In the fall, she told a counselor at school that she planned to kill herself; she was quickly re-admitted to the same inpatient unit, given priority as a former patient, and spent two weeks there. When her stay ended, G went into an intensive outpatient program. But a counselor there told her mother that G needed more intensive care because she had described a plan to kill herself.
“They told me, ‘This kid is on fire, she’s too acute to be here,’” G’s mother recalled. This time, the family went to the emergency room at a different Boston-area hospital, Salem Hospital, where G boarded only one night and, this time, was lucky to get a bed in that hospital’s inpatient unit, where she spent three weeks, until mid-October.
G’s mood these days is “better than it was, but it still sucks,” she said recently. And, she added, “I’m better at covering things up more.”
“Once people ask you a question, ‘Do you feel suicidal,’ you have to say nope,” she said. “You can’t tell them anything or they’ll send you to the hospital.”
Matt Richtel is a best-selling author and Pulitzer Prize-winning reporter based in San Francisco. He joined The Times in 2000, and his work has focused on science, technology, business and narrative-driven storytelling around these issues. @mrichtel
By Kathy Rivera, published in Anton Media, May 27, 2022
North Shore Child & Family Guidance Center is known throughout Long Island as the preeminent mental health organization for youth and families, providing individualized, culturally sensitive therapeutic services that serve to bring hope and healing to those experiencing mental health challenges. For nearly 70 years, the Guidance Center has been listening to your needs and concerns, and responding swiftly and compassionately. Since May is Mental Health Awareness Month, we wanted to share with you some important information on our offerings.
As we told you in our April Anton column, we shifted to a hybrid model of service within days of the pandemic’s beginning, seeing clients both in person and via a secure telehealth platform.
But if you picture the work of the Guidance Center as taking place only inside our three buildings or via a virtual platform, with a counselor and client sitting in an office or communicating via a smartphone or computer, think again. Many of our innovative programs happen beyond our walls, in places that range from state parks to schools to homes.
The Guidance Center’s Wilderness Respite Program, now in its 23rd year, provides a unique opportunity for at-risk adolescents to put down their tech devices and participate in hikes and other nature activities that help them gain confidence and make lasting friendships.
Nature takes a leading role in our two Organic Gardens, located at our main headquarters in Roslyn Heights and our Marks Family Right from the Start 0-3+ Center in Manhasset. By weeding, seeding and tending to the crops, kids blossom as they learn important skills such as self-confidence, cooperation and responsibility.
The Guidance Center also has a Nature Nursery, where our youngest clients use all their senses as they touch pinecones or paint on an outdoor “canvas.” The textures, sounds and sights help children explore their creative sides and learn skills to help cope with difficult feelings.
In addition to therapy, our Latina Girls Project incorporates monthly outings to places such as theaters, museums and more. These trips boost the teens’ confidence and sense of independence and help them discover the larger world. In 2019, the trips expanded to include outings for boys that also have been a huge success.
Students from 5-21 who’ve had a hard time succeeding in school have a great alternative with our Intensive Support Program (ISP), held at three Nassau County B.O.C.E.S schools. There, they receive academic help and counseling, with therapists on site to help them flourish emotionally and academically.
We also work in Westbury high school and middle school with our Teen Intervene and Too Good for Drugs programs, designed to prevent substance and alcohol use.
For children and teens who need our help but can’t come to our offices, the Guidance Center provides intensive in-home therapy with our Clinical Care Coordination Team (CCCT). CCCT aims to lessen acute symptoms, restore clients to prior levels of functioning, and build and strengthen natural supports. Through CCCT, our goal is to reduce unnecessary emergency room visits, hospitalizations and residential placements.
Our Coordinated Children’s Services Initiative (CCSI) supports families with the coordination of services in their homes and communities, identifying and accessing resources, providing advocacy and helping children and families gain the skills and tools needed to be self-sufficient.
Through our Family Advocate Program, parents who have been through mental health crises with their own children are trained to offer peer support for families by joining them at special education meetings, offering support groups and providing many other resources.
As you can see, the Guidance Center is always thinking “outside the box,” creating innovative programs that meet the needs of the community and enhance the therapeutic value of all our services. We are here for you!
Bio:Kathy Rivera, LCSW,is the Executive Director/CEO of North Shore Child & Family Guidance Center, Long Island’s leading non-profit children’s mental health organization. To get help for your child or to support the Guidance Center’s lifesaving work, call (516) 626-1971 or visit www.northshorechildguidance.org.
Having a child on the autism spectrum brings about an array of emotions. You have your good days and bad days. You probably already know that certain experiences, like moving, require careful consideration and understanding. If you need pointers to help make your upcoming move as smooth as possible, spend a few minutes reading the following guide presented by North Shore Child & Family Guidance Center.
Make the Experience a Positive One
Your child may struggle with change, especially sudden changes. Let your kid know as soon as you can that you’re planning to move. Introduce the subject calmly. Explain to your child why you’re moving and how wonderful the experience can be. Incorporate your child in the moving process as much as possible, such as by helping pack boxes.
Research the Market
Before you start looking for a house in Roslyn Heights, research your target market. Discover how much the average home costs.
Use this information to determine how much you can spend on a home. Look into grant programs that may help you with the cost of home modifications for children with autism.
Consider choosing a house with a fenced-in yard, or think about hiring a fence installer to add one. Make sure you look at schools and parks in the area, too.
Make a Calming Space for Your Child
You’re probably already experienced a number of meltdowns during your time parenting your autistic child. These emotional outbursts are a reaction to too many stimuli.
By creating a calming space in the new house, your child will have an area they can go to when the world becomes too much.
Think about your child’s sensory needs. You’ll more than likely want light-blocking curtains. Walls should be a light color, nothing too bold, dark or bright. Gather a collection of sensory toys, such as water beads or fidget toys.
Declutter and Clean
As you’re in the process of moving, make sure you’re decluttering and cleaning as you go along. You’ll make life simpler by reducing clutter. Not only can clutter make you feel overwhelmed, but it can also affect your child negatively as well.
As you sort through the items, get rid of duplicates or anything you haven’t used in a year. If you notice something has collected dust, it’s probably safe to toss it. Considertaking photos of nostalgic items rather than keeping them all.
If you notice you have an upholstery stain that you’ve unsuccessfully battled using store-bought cleaners, contact a professional upholstery cleaner to contend with the blemish. You’ll reduce your stress so you can focus on your child, you, and the move.
As you’re searching for an upholstery cleaner, look online for reviews to compare. Choose a few that have the highest ratings and schedule meetings. Make sure you discuss your needs and get quotes. Ask for referrals from previous clients. As a general rule, you should avoid companies that use all-in-one cleaners.
By following some of these tips, your child will have a much easier time moving—and so will you!Bio: Jenny Wise created Special Home Educator as a forum for sharing her adventures in homeschooling and connecting with other homeschooling families. She has been homeschooling her four children for many years now, including her youngest daughter Anna who is on the autism spectrum.
By Kathy Rivera, published in Anton Media, April 27, 2022
As of this writing, while COVID-19 cases have been inching up, most experts say that we have moved into a new phase of the pandemic, where the disease, while still dangerous, is less deadly than previous strains. In addition, preventative measures and treatments have advanced far beyond the early days of the crisis, when so little was known.
Certainly, that is news we’ve all been hoping to hear for more than two years, but there is another crisis that shows no signs of abating: the epidemic of mental health issues spurred by long-term social isolation, anxiety, illness, financial insecurity and other challenges.
While all of us have been impacted, the reality is that children, teens and young adults have experienced the losses surrounding COVID-19 in deep and potentially long-lasting ways. Numerous studies have reported sharp increases in rates of depression, anxiety, loneliness and suicide attempts. In addition, the number of U.S. children who have a lost a parent or other caregiver to COVID-19 is estimated to exceed 200,000.
In a first-of-its-kind study of youth mental health during the pandemic period, released on March 31, 2022, the Centers for Disease Control and Prevention reported a dramatic increase in emotional and psychological trauma in kids and teens. More than a third of high school students said they experienced poor mental health during the pandemic, with 44% reporting they felt “persistently sad or hopeless.” One in five considered suicide, and nearly 10% made a suicide attempt.
The CDC also reported that, during the first seven months of lockdown, hospitals experienced a 24% rise in mental-health-related emergency visits for children aged 5 to 11, and a 31% increase for those aged 12 to 17.
Sadly, these statistics came as no surprise to the team of clinicians at North Shore Child & Family Guidance Center (the Guidance Center).
From the early days of the pandemic, we have been flooded with calls from hospitals, emergency rooms, urgent care centers, parents, schools and others desperate for help as they saw those statistics come to life.
At the Guidance Center, we’ve provided therapy to children—some as young as three years old—who are experiencing deep grief from the loss of a parent or other loved one. Many are grieving a loss of hope and confidence about their futures. Others are in dire financial situations born of pandemic job loss. All lost fundamental things that we used to take for granted: the ability to be with friends, go to school, celebrate joyous occasions, participate in extracurricular activities and have confidence that we were safe in the world.
Even if the pandemic disappeared tomorrow, the mental health effects would not disappear with it. Unfortunately, we cannot expect our children to simply get over what has been such a profoundly difficult, scary and uncertain time.
Despite these gloomy predictions, parents need not succumb to hopelessness. You have a vital role to play, and it’s one that can make all the difference in helping your children survive and even thrive despite the challenges of the past two years.
First, be on the lookout for signs of emotional distress. Is your child or teen isolating themselves, even though they are allowed to be with others? Have their sleeping or eating patterns changed? Have their grades dropped dramatically? Have they lost interest in the things that used to make them happy? Are they more irritable than usual? Have they turned to substances to improve or numb their moods?
Don’t assume that they will tell you they’re struggling. Ask them how they are feeling. Assure them that it’s normal to be feeling sad, scared and even angry in the face of all they’ve experienced. And tell them there is absolutely no shame in asking for professional help. Tell them, it’s OK not to be OK.
The Guidance Center has been serving the community for nearly 70 years, and we are here during this time. We never turn anyone away for inability to pay, and we promise to see urgent cases within 24 to 48 hours through our Douglas S. Feldman Suicide Prevention Project and our Fay J. Lindner Foundation Triage and Emergency Services. We offer individualized, culturally sensitive treatment via telehealth, in person or a combination of both, depending on the needs of the family.
Children are not little adults. They have specific needs that are best addressed by mental health professionals who are specially trained to help young people. They are also resilient, and with the proper support, they will overcome the challenges brought on by the pandemic. We all will.
Bio:Kathy Rivera, LCSW,is the Executive Director/CEO of North Shore Child & Family Guidance Center, Long Island’s leading non-profit children’s mental health organization. To get help for your child or to support the Guidance Center’s life-saving work, call (516) 626-1971 or visit www.northshorechildguidance.org.
At North Shore Child & Family Guidance Center, the well-being of children and families always comes first.
At the legal practice of John M. Zenir, Esq., where the focus is on family law, divorce law and estate planning, the exact same philosophy holds true.
“Children are deeply affected by divorce, custody, abuse and other difficult circumstances,” says Zenir. “One of the realities with family law is that kids always think they caused the problem between their parents; whether they are 2 or 22, they believe it’s their fault if their parents are getting divorced.”
Improving the lives of children has been central to Zenir’s life. As a young man, he taught 7th and 8th grade, and helped young people receive their high school equivalency diplomas.
While he veered from that path for nearly two decades, running a family cleaning supply business, he eventually found himself drawn to the law and got his degree at Touro. He soon felt pulled to center his practice around family law, working for many years representing children as part of a law guardian panel.
Therapy is Vital
His experiences in family court gave Zenir an unvarnished look at what conflict in the family can do to children. “When I first started as a lawyer, I saw how difficult it was for children to witness their families breaking apart,” he says. “It was devastating.”
But at the time, he adds, there was little open discussion about therapy. “Receiving mental health care is essential when kids go through such challenging times,” says Zenir, who shares that mental health issues in his family impacted him as a child. “It’s so important that we make therapy available to young people. That way, we will be much more likely to create adults who are not limited by their traumatic childhood experiences and can deal with society’s problems.”
The Children’s Center
Zenir’s involvement with the Guidance Center began when we took on the role of overseeing the Children’s Center at Nassau Family Court, which was designed to provide care and early learning to children, ages 6 weeks to 12 years, while their parents or guardians were conducting court business.
Since the pandemic took hold, family court has moved to an almost exclusively virtual model, so the Children’s Center has not operated for the past two years, but its value to the families who used it over many years is unquestionable.
“It gave families the freedom to not worry about what their children might experience if they had to wait in a hallway near the courtroom,” says Zenir, who co-chaired many fundraisers for the Children’s Center with Robert C. Mangi, Esq. and Allison Cacace.
The Children’s Center, founded by the late Honorable Burton S. Joseph, was loved not only by kids but also lawyers and judges.
“Family court issues can be contentious and highly emotional, and yelling and angry outbursts aren’t uncommon,” says Zenir. “Before the Children’s Center existed, kids were at risk of hearing adult conversations that they shouldn’t hear, which made court officials very concerned. It served to protect children from heated exchanges, and the people running it from the Guidance Center were wonderful.”
Championing Our Mission
Zenir continues to be a champion for the Guidance Center. He recently began charging a $100 consultation fee to prospective clients, which he donates in full to support our work.
“Especially during pandemic times, there is no question that kids desperately need therapy,” he says. “Everyone is recognizing that therapy is a big part of wellness today, and that the more available therapy is, the better our community will be.”
What the Future Holds
While Zenir’s practice is thriving, he’s considering reducing his hours so he can spend more time with his wife Deborah of 52 years, his three children and six grandchildren—but he doesn’t expect to ever retire fully.
“I will probably cut down to 16 or 20 hours somewhere down the road,” says Zenir, a history buff who plans to travel more and increase his visits to the New York Historical Society.
Whatever path he chooses, the Guidance Center is grateful to John Zenir for his unwavering dedication to the children and families of Long Island and to the Guidance Center’s vital work.
To learn more about supporting North Shore Child & Family Guidance Center, contact Director of Development Lauren McGowan at (516) 626-1971, ext. 320.
For parents whose children experience serious emotional and behavioral issues, the challenges can seem overwhelming. Not only are they dealing with the stress and heartbreak of seeing their kids struggle, they’re also trying to navigate a complex maze of services related to school, health, housing, finances and more.
These families often don’t know where to turn—plus, they can feel desperately alone.
North Shore Child & Family Guidance Center has an innovative program that addresses the needs of these caregivers: our Family Advocate Program which pairs parents with one of our family peer advocates.
“These credentialed professionals aren’t therapists,” explains Paul Danilack, Supervisor of High-End Community- Based Services at the Guidance Center. “Rather, they are parents of their own children with special needs who are trained to educate, guide and empower other parents to better understand their children and their needs.”
“We want to help these parents not feel so isolated.”
For two decades, Yvonne Novy-Cutler has been a family peer advocate with the Guidance Center, meeting with parents to learn about their child’s particular issues, which may include severe depression and anxiety, school refusal, aggressive behavior and more. “Whereas social workers and mental health counselors work with families, we can share our personal experiences,” she says. “We’ve been where they are and have walked in their shoes.”
Family peer advocates provide a wide range of support, attending evaluations with parents; going to CSE (Committee on Special Education) meetings; helping build skills within the family to manage difficult behaviors; and seeking residential placement or inpatient hospitalization if needed. While advocates don’t provide therapy, they can help families access those services.
Shari Bushansky, another one of our dedicated advocates, helps run the program’s weekly support groups, where parents share their challenges and successes, talk about what worked and what didn’t, and build a social support network.
“We want to help these parents not feel so isolated,” says Bushansky, who has been serving our clients for 20 years. “Often, their family and friends don’t understand what it’s like to be the parent of a child with emotional and behavioral disabilities, and it helps the parents to know they aren’t alone.”
Our advocates work with parents and the child’s therapist to help design a plan to modify their youngster’s negative behavior. For example, they help parents create behavioral charts to develop a uniform approach of rewards and consequences, which helps motivate children to listen and respond appropriately. Moreover, advocates act as a bridge to many services, such as schools, counselors, courts, case management and others.
Danilack has nothing but praise for his team. “Yvonne and Shari are critical members of both the department and the agency,” he says. “They put their all into their work and know better than anyone how to connect with the families they serve.”
Both Novy-Cutler and Bushansky say that, while their work can be stressful, the rewards far outweigh the difficulties. “These parents have been down a long, tough road, and watching as their families heal makes it all worth it,” says Novy-Cutler. Confirming the advocates’ value at a recent parent support group, one mom stated, “These two women have saved my life!”
This story will be published in Blank Slate Media newspapers in April 2022
Helping Your Child Through Divorce
In this monthly column, therapists from North Shore Child & Family Guidance Center answer your questions on issues related to parenting, mental health and children’s well-being. To submit a question, email communications@northshorechildguidance.org.
Question: After much discussion, including couples therapy, my husband and I have decided to divorce. We both know it’s the right thing to do, but we’re very worried about how our kids (we have two girls and a boy, 5, 8 and 10) are going to handle it. Can you offer some advice on how we can best support them during this difficult time?
— Splitting Up
Dear Splitting Up:
The rise in divorce rates in the pandemic period show that you and your husband are far from alone: In 2021, the COVID-19 crisis triggered a nearly 21% increase in divorce filings compared with the previous year.
Whenever there is a separation or divorce, there is no way around the fact that your children will be impacted in profound ways.
And, while divorce doesn’t have the same stigma it did years ago, it still is a difficult event in a young person’s life.
The dissolution of their parents’ marriage can create enormous stress for youngsters. Divorce can be devastating to the children’s feelings of safety, causing fear of abandonment and fear of losing a parent’s love. The result: Anxiety, depression and low self-esteem are common.
Guilt is often another problem, as many children blame themselves for the divorce, believing that it is somehow their fault and that if they had just been “good,” the separation never would have happened.
In addition, many parents make the mistake of talking negatively about their ex-spouse in front of their children. This upsets them because they see their parents as their caretakers, and they need to feel safe and supported by both of them.
When parents put their kids in the middle of their battles, the children struggle with issues of loyalty. Even if they are very caring parents, they may do things inadvertently that cause distress to their child, such as asking the child to talk with the ex-spouse about a change in weekend plans instead of dealing with the adult directly.
Here are some tips on how to help your children deal with divorce:
Be supportive, reassuring your kids that both of you will always love them and be there for them.
Encourage them to speak to you openly about all their feelings, and validate that those feelings are normal and completely acceptable.
Learn how to co-parent the children so there is no confusion on discipline. Rules about bedtime, homework and the like should remain consistent.
Never talk negatively about the other parent in front of the children.
If possible, show a united front by attending events like back-to-school nights, games and other activities together.
Let their teachers know about your separation so they are on the lookout for any troubling behaviors from your children.
Foster the relationships your children have with your ex’s family so they don’t feel the loss of those attachments.
Consider placing your child in a therapeutic group so they don’t feel like they are alone in their experience. Many schools have programs like “Banana Splits” offered by school-based social workers.
Be sure to get support for yourself through this process through friends, family members and professional therapy, if needed.
Remember, the post-divorce relationship with your ex-spouse is perhaps the most important factor in how well your children handle the matter, so do your best to get along for their sake. Knowing that they are loved no matter what by both of you is the most important message. During the pandemic, North Shore Child & Family Guidance Center is seeing clients both in person and remotely via a telehealth platform. To make an appointment, call (516) 626-1971 or email intake@northshorechildguidance.org.
The COVID-19 pandemic has had a staggering impact on nearly every aspect of our lives, but one of the pandemic’s most notable and long-lasting effects has been the increasing rates of burnout in the United States. While burnout—a type of exhaustion caused by exposure to prolonged or repeated stress—is often discussed in the context of the workplace, it can affect everyone. From office employees to students to caregivers, burnout is taking a significant toll on our mental health.
Traditionally, burnout is understood in relation to stress at work. In 2019, the World Health Organization first declared workplace burnout a “stress syndrome.” The symptoms include “feelings of energy depletion or exhaustion” and “reduced professional productivity.”
But burnout in settings other than the workplace has drawn further attention in the past two years. Caregiver burnout is described as a state of “physical, emotional and mental exhaustion.” When schools transitioned to remote learning in 2020, many parents and caregivers struggled with a sense of burnout due to the added responsibilities at home. Psychology Today notes that burnout often occurs when someone “is not in control of how a job is carried out.” The lack of control that we have all experienced amid the pandemic’s unpredictability is likely a major cause of increasing rates of burnout.
School Pressures Can Create Burnout
Students of all ages are also facing academic burnout, especially alongside the challenges of remote learning and the other emotional burdens brought on by the pandemic. But it’s not a new experience. Even before the pandemic, high school students felt a heightened weight on their academic performance in the face of the college admissions process. Similarly, college students felt that their career opportunities and future success might be hindered by any academic difficulties.
One of the most troublesome parts of burnout is that we often do not recognize it when it is building within us. Caregivers are often so focused on those dependent on them that they neglect to pay attention to their own well-being, instead prioritizing the needs of others. Similarly, students may prioritize their productivity and responsibilities, even outside of the normal school day or week, and they don’t take time to rest.
However, by prioritizing our productivity and neglecting our mental and physical well-being, we often sabotage the very productivity we sought to protect. Once stress transforms to burnout, the negative impact on productivity is inevitable. For caregivers, the old adage of caring for yourself before caring for others is important to keep in mind. We must help ourselves to help others.
The Need for Self-Care
One of the most important ways to prevent burnout is to regularly engage in self-care. Though we often see self-care portrayed in the media as expensive skincare products or a rigid exercise program, the most effective methods are often the simplest. By identifying small activities that bring you the most joy, you can find simple ways to incorporate self-care into your daily routine.
This may mean choosing to listen to your favorite song on your commute to work, going for a morning run, or calling a loved one at the end of the day. The easier it is to include in your schedule, the more likely it is that you will make it a true habit.
In a similar vein, mindfulness can help to prevent burnout by reducing stress and improving boundaries between yourself and your work. Thirty-minute mindfulness exercises such as meditation or journaling can be added to a daily routine relatively easily. However, these exercises are not for everyone. Mindfulness can be incorporated, instead, into the activities in which you already engage. Mindfulness, above all, is a heightened sense of awareness and presence. To increase this, you may decide to put your phone away while eating lunch so you can focus solely on your meal or to take a walk without listening to anything but the sounds s of nature around you.
Emotional self-care, above all else, must bring you joy. It should not feel like yet another burden or responsibility to bear. Allow yourself to think outside of the box. Self-care does not look the same for everyone.
As we continue to navigate our lives amid the effects of the COVID-19 pandemic, it is important that we take this as an opportunity not to panic about the impact of burnout but instead to prioritize self-care and overall well-being. This awareness of burnout, ultimately, will serve as a time of revolution and innovation in work, caregiving, academics and all other aspects of our lives.
Bio: Kelly Christ is a guest blog writer originally from Manhasset, NY. Kelly is currently studying social work at Fordham University’s Graduate School of Social Service in New York, NY. She received her bachelor’s degree at Fordham University at Rose Hill in 2021, where she double majored in English and Psychology. Kelly is passionate about both writing and mental health advocacy.
At North Shore Child & Family Guidance Center, our mission is to bring hope and healing to children and families experiencing depression, anxiety and other challenges. Although we are a children’s mental health organization, we know that emotional well-being and physical health are inexorably tied, each deeply impacting the other.
The Guidance Center has several programs that promote the health of mothers and children. One is our Good Beginnings for Babies program, which aims to promote healthier pregnancies that will result in healthier babies and to nurture relationships between parent and child. Good Beginnings for Babies supports teen and young adult mothers prior to the birth of their child and throughout the first year of the child’s life with support, counseling and advocacy.
Through our Diane Goldberg Maternal Depression Program, we provide a rapid response and diagnosis for mothers suffering from postpartum depression and other perinatal mood and anxiety disorders, which are estimated to impact one in seven women.
As part of our educational and advocacy work, the Guidance Center partnered with Hofstra University’s Public Health Program, School of Health Science and Human Services to create Birth Justice Warriors, an initiative born out of the crippling bias and injustice faced by Black mothers in the United States in general and in Nassau County in particular.
According to the New York State Department of Health, a Black woman is up to four times more likely to die in childbirth than a white mother. In Nassau County, the infant mortality rate per 1,000 live births is 9.4 for Black babies versus the 2.2 reported for white non-Hispanic babies.
Birth Justice Warriors are volunteer advocates from many professions and backgrounds, working with community members, pediatricians, nurses, health care professionals, elected officials, members of faith-based institutions and others to bring education and awareness to this inequality. Ultimately, one of Birth Justice Warriors’ goals is to have legislation written that guarantees that this crucial information is delivered to all women of child-bearing age.
In late January, I joined with Dr. Martine Hackett, my Birth Justice Warrior co-founder and an associate professor in the public health and community health programs at Hofstra, at a press conference held by New York Senator Kirsten Gillibrand. The senator, along with Representative Alma Adams of North Carolina, are the sponsors of the Maternal CARE Act, which would provide funding for evidence-based training programs to reduce bias in maternal health and establish programs to bring health care services to pregnant women and new mothers in an effort to reduce the disproportionate rate of maternal death and other poor health outcomes among Black women and their babies.
In her statement, Gillibrand said the following: “Health equity for Black women can only happen if we recognize and address persistent biases in our health system and do more to ensure women have access to culturally competent, holistic care to reduce preventable maternal mortality.”
Both North Shore Child & Family Guidance Center and Birth Justice Warriors support this important legislation, and we hope that you will join us in spreading the word so that allwomen receive the care they need and deserve.
Dr. Nellie Taylor-Walthrust is the Director of North Shore Child & Family Guidance Center’s Leeds Place and is a co-founder of Birth Justice Warriors, a collaboration of the Guidance Center and Hofstra University. To learn more about Birth Justice Warriors, contact Dr. Walthrust-Taylor at (516) 997-2926, ext. 229, or email NTaylorWalthrust@northshorechildguidance.org.
Ashley Rivas had to grow up fast during the pandemic.
At age 15 in early April 2020, she shielded her 8-year-old sister from the details of their mother’s hospitalization due to COVID-19, a newly known virus that also had forced schools to close statewide.
When their mother was in the hospital, the teen helped her father sanitize the house and washed clothes for the family. She also took on the role of caretaker for her sister, helping her with homework in between their online classes. After her mother was released from the hospital two weeks later, she brought her food and cared for her while she was recovering.
“I was trying to keep my house together with my mom being sick and trying to be the next her,” Rivas, a Hempstead High School senior, recalled.
Rivas, now 17, is expected to be among about 35,000 Long Island students graduating in June, representing a milestone for a class that has weathered two years of pandemic learning. The students Newsday spoke to said they matured faster during the pandemic, when they had to take care of family members sickened with the coronavirus, and became more disciplined because of their virtual and, later on, hybrid schedules.
Some seniors said they have gotten back to normal since the school mask mandate ended on March 2. They look forward to resumed field trips, get-togethers with friends, the prom, graduation and adulthood. Others noted school is still not the same amid the uncertainty, lamenting lost opportunities to grow friendships, along with the missed basketball games and concert rehearsals that could not to be rescheduled.
Dena Papadopoulos, a mental health counselor at Roslyn Heights-based North Shore Child & Family Guidance Center, said this senior year has been marked by amplified excitement, but also anxiety.
“There is that … general anticipatory anxiety that ‘I’m excited for college’ or ‘I’m excited about the next step,’ but ‘I’m also anxious because I don’t know exactly what to expect’ ” in any given senior year, she said. Now, “It’s more intensified.”
‘Stronger than I thought I could be’
In the spring months of 2020, Rivas was struggling.
“The teachers didn’t really know how to work with Zoom; my mom was in the hospital, I think. And then it was also around my birthday,” she recalled. “Everything was just falling apart.”
Because school was virtual and New Yorkers were urged to stay at home, Rivas found herself with a lot of alone time.
One day when scrolling TikTok, she saw people crochet. She had never done it before but decided to give it a try. She bought some yarn and watched tutorials online. Soon enough, she made a bee plush and put it on Etsy. It sold the next day. She sold about 20 more later.
Rivas always has been interested in business. When she was a first-grader, she sold purses made out of duct tape to her classmates for $3 apiece. She also has considered becoming a schoolteacher like her mother did in her home country of El Salvador.
Her bee plush success helped crystallize the path she wants to take. Rivas said she plans to study business administration or economics for her undergraduate degree, though she’s yet to choose a college. National College Decision Day is May 1.
The experience also taught her something else.
“I think I matured a lot quicker,” she said. “It made me realize that maybe I hadn’t known who I really was. There were parts of me that I didn’t even know about. … I’m stronger than I thought I could be.”
To protect her mother, who still has a dry cough, Rivas continues to wear a mask in class for the most part.
“It’s still not the same,” she said of school. “It’s always in the back of your mind that there’s a global pandemic going on. And you have to be careful.”
Had to become a ‘mini adult’
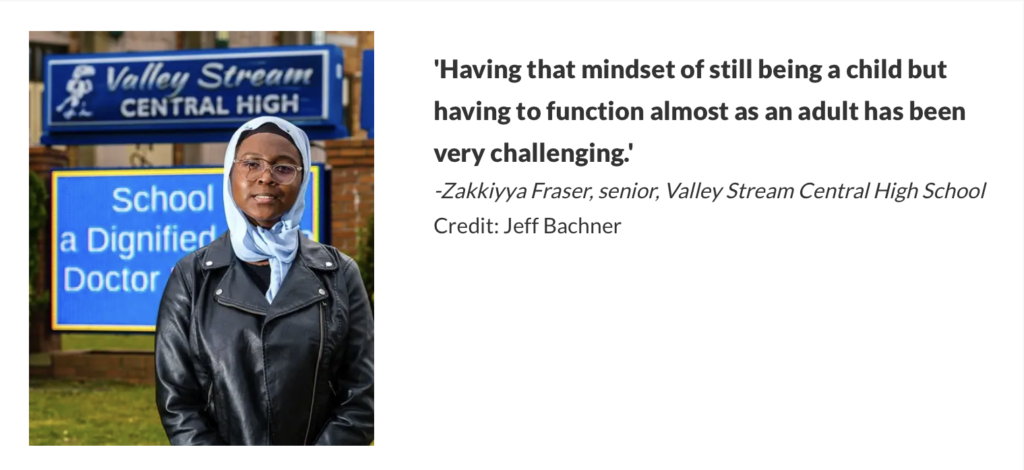
Zakkiyya Fraser, 17, a senior at Valley Stream Central High School, remembered looking to adults for answers in the early days of the pandemic.
And not getting them.
It took Fraser some time to learn to accept the unknown. “It’s like you become a mini adult,” she said.
“The pandemic may have made us grow up in a [different] way,” she added. “Having that mindset of still being a child but having to function almost as an adult has been very challenging, I think, for all high school students.”
When school turned remote and, later on, hybrid, Fraser said she pushed herself to become more independent. The routine structured by a typical school day was no longer there, and the inconsistency of learning online was difficult for her to adjust.
“Being on the computer is like, not necessarily that you’re forgotten, but much harder to connect in the classroom,” she recalled. “It’s harder to grasp the content. It’s almost like you’re there, but not there.”
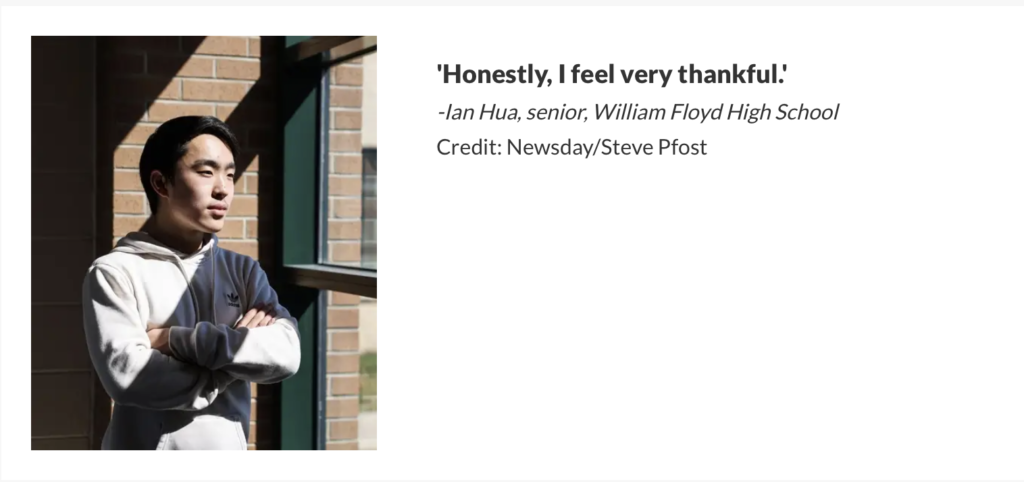
Ian Hua, a William Floyd High School senior, can relate.
“We didn’t have a school schedule to keep us on track. We needed to manage our own time without a bell,” the 18-year-old said. “We didn’t have teachers to ask questions to. We did, but it was much harder to communicate.”
Still, Hua said he feels “overwhelmingly lucky” compared to other student cohorts who were affected by the pandemic differently.
“There were seniors that had their final events taken away. They had no prom. They had no graduation,” Hua said. “Then there are younger kids that never had a first year of kindergarten. … Honestly, I feel very thankful.”
Shifting his perspective
Timothy Hogan, a senior at East Islip High School, didn’t begin to appreciate school until it was shut down.
Before, it was like “you can’t wait to leave,” the 17-year-old said. “With COVID, it made me want to go to school in person.”
The pandemic also has taught him that the things he used to not give a second thought are not a given.
“Whether it’s family, school, your friends, going out to see a movie or to shop, you can’t take those things for granted,” Hogan said.
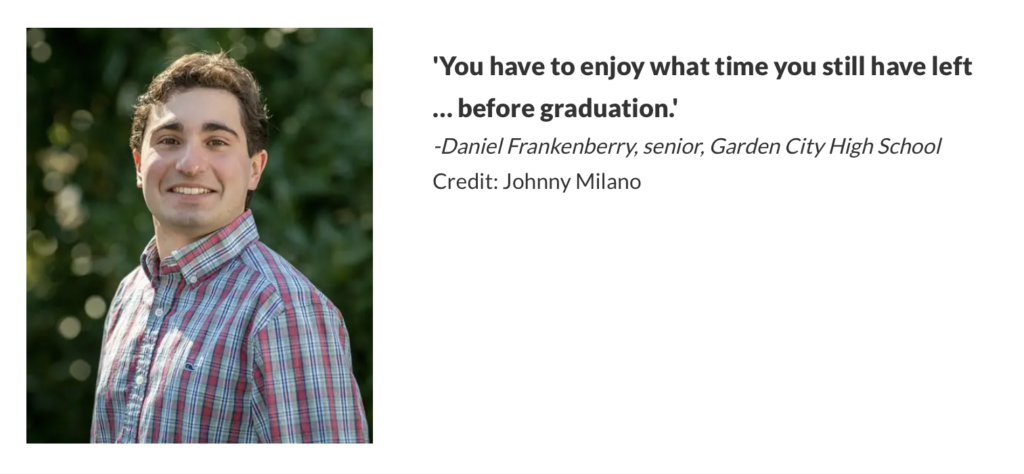
Sharing similar sentiments, Daniel Frankenberry, 18, said he grew closer to his family.
Those first few months of staying at home allowed him to spend more time with family, an experience that confirmed his desire to stay in or near New York when choosing a college. “It reinforced the idea that I wanted to stay home,” he said. He’s yet to decide which college to attend.
Looking back, Frankenberry felt like part of his high school years was stolen.
The better part of “my second half of sophomore year just didn’t exist,” the Garden City High School senior said.
His junior year was spent under such heavy restrictions — plastic shields around desks, social distancing and masking — that he said regular interactions were greatly reduced.
“It’s unfortunate,” Frankenberry said. “Definitely a little bit upsetting. It’s a shame that [we] couldn’t get the full experience.”
Frankenberry is hanging out with his friends as much as he can and planning social activities — almost as if to make up lost time.
“I can’t say I’m trying to fix everything,” he said. “You’re not going to be able to make all that time back. But you have to enjoy what time you still have left … before graduation.”
March is National Social Work Month, and today happens to be World Social Work Day! Every day of the year, we are proud of the dedicated staff at North Shore Child & Family Guidance Center, which consists of social workers, mental health counselors, psychologists, psychiatrists and other mental health professionals, all of whom work to bring hope and healing to the children and families in our community – more important than ever during the pandemic, which has created a true mental health crisis.
Here, some of our staff members give insight into their chosen careers:
“I like to say that the social work profession actually chose me instead of the other way around. Through my own personal experiences with trauma, abuse and neglect, I needed to find a way to heal and experience an inner serenity. The social work profession has given me the tools to help combat and overcome many challenges throughout my life. I enjoy being able to help others, and it was clear to me early on in my career that changing the world starts with helping one person and being able to empathize with them. I have been in their shoes. North Shore Child & Family Guidance Center is a place of hope and healing for so many of our children and families. That’s the reason I am here and love to do what I do.”
Kathy Rivera, LCSW, Executive Director/CEO
“Although I’ve known this for a long time, the past few years have reinforced that social workers are the most dedicated, selfless and courageous people out there. Social workers get the job done. They show up day after day providing guidance, hope and support to others, often with the thought of wishing they could do more. And while social work practice is undervalued in society, social workers aren’t doing this work for acknowledgement or compensation. They recognize that making a difference for one child or family is important enough to keep going. I am grateful to be part of a team of compassionate, talented clinicians and hope that we continue to show the world who we are and what we do. Happy Social Work Month!
Vanessa McMullan LCSW
“My primary mission in choosing my career path was to try to enhance people’s well-being with particular attention to the needs and empowerment of those who are vulnerable, disenfranchised, oppressed or at risk. I have a personal and professional passion for working with at-risk youth and those in need, helping them find their strengths and ways of looking at the world from a different lens and showing them ways of being that they may have never thought were possible.”
“Dee” Nendler Michel, LCSW
“I am a licensed psychologist back home in Venezuela, and when I immigrated to the United States, I decided to rebuild my career and became a social worker. Working with children and families has been my passion in the past 20 years. I strongly believe that intervening in families creates a better foundation for societies. Working with Spanish-speaking children and their families ensures a better future for this community, my community.”
Erika Perez-Tobon, LMSW
“I always knew I wanted to help others, and while I was going through the college application process, I decided to study psychology as an undergraduate. While there, I spoke with professors and completed an internship in the mental health field. Ever since then, I knew this was the career for me. So many children and families are in need of assistance and are doing the most they can for support. It has become my pleasure to work with and advocate for these children and families.”
Paul Danilack, LMHC
“Adolescence is a time of great change, both emotionally and physically. I have always been fascinated about how this turmoil eventually gives way to adulthood. There are many detours along the way, and oftentimes youngsters need help ‘steering their ship’ or even preventing it from ‘capsizing.’ I very much enjoy being part of this journey. Having once been an adolescent myself (some would say I am still one!) I feel I have a lot to offer in easing pain, perspective and support. I enjoy helping to turn chaos into harmony and the valuable lessons that I learn from interactions with my young patients.”
Dr. Jolie Pataki
“I chose to be a social worker because I was lucky enough to be raised by one! My mom, who has been a clinical social worker for over 35 years, always said to me, ‘You are such a natural social worker!’ As it became time to choose colleges, I had already known in my heart that social work was what I wanted to do for my career. This is not, nor has it ever been, simply a job or career for me. This has been my passion. Putting a passion and a career together is a uniquely beautiful thing. I always wanted to help. I always want people to feel safe, heard, respected and validated. I always wanted to help people find their voices.
It has been truly rewarding to work with children and their families because you get to watch them grow. You get to be a part of their story. You get to help them in their most vulnerable moments, which I feel are the moments that show the most strength. They allow you into their lives in such a unique way. When clients learn their own strengths (that you saw from the moment you first interacted with them), that is why it is so rewarding. The human connection and allowing their pain to be kept safe with you is an honor.
Starting as an intern, now being a Clinical Supervisor of this agency, with our mission being ‘restoring and strengthening the emotional well-being of children and families’ is truly rewarding.” Gillian Uhl, LMSW
“I got into social work due to my mom being a social worker. I grew up in a multicultural home as she was a host mom to international students through the University of South Carolina at the time. I learned early on that helping others was a part of life and only enriches your life. I also remember telling my mom while I was in graduate school that I don’t need a degree to help people.
Now that I am in the profession for three years, I have been able to grow my skills and see the potential that this profession has. The experiences I have had at the Guidance Center have set me up for anything the world has to offer. I know its cliché, but I really feel like I have saved lives doing what I do. Being in the drug and alcohol program, you get to experience the lowest points of youth as they utilize substances to cope. To bring people out of that place so they can see the light within themselves to do better and be better is beyond words. Helping them learn to love themselves amid all the traumas they may have been through highlights their own ability to make it through anything. It is this part of the profession that keeps me going. Incorporating mindfulness practices such as meditation and deep breathing has been the cornerstone of my style. Incorporating them into garden therapy would be the next step in my journey and what I’m actively working toward.”
Ricardo Castillo, LMSW
My journey into the mental health field began with having a parent who was a middle school guidance counselor and was very attuned to addressing feelings. I always knew that this too was my passion and direction in life. For me, I enjoy working with a multidisciplinary team of outstanding dedicated professionals who all have a similar goal in mind, the health and well-being of children and their families. It’s very rewarding to work with families to shift to a more positive perspective for their child and see that child on a more successful path emotionally, behaviorally and educationally.
In this monthly column, therapists from North Shore Child & Family Guidance Center answer your questions on issues related to parenting, mental health and children’s well-being. To submit a question, email communications@northshorechildguidance.org.
Question: I have two daughters, 9 and 13 years old. While my youngest tends to approach life with a laid-back attitude, my older one has always been prone to anxiety. Even before the pandemic, she was having panic attacks, but they’ve gotten much worse in the past two years. I had hoped that the return to school and other “normal” activities would help, but it’s gotten so bad that she is avoiding social situations and spending most of her time in her room. How can I help her get over her anxiety?
–Parent Puzzled by Panic
Dear Parent Puzzled by Panic: Anxiety is a normal part of life, for both kids and adults. It would be difficult to find a child who, at some point, didn’t worry about monsters in the closet, or feel apprehensive on the first day of school. Moreover, the last two years have heightened feelings of anxiety for everyone, with the losses, fears and other difficult emotions that have arisen from the pandemic.
In most cases, children’s anxieties are eased with reassurance, love and comfort from an adult in their lives. But for some young people, anxiety is a constant companion. It is part of their everyday lives, and it can seriously impair their functioning. It can lead to debilitating panic attacks, which are characterized by symptoms such as shortness of breath, shaking, dizziness, heart racing and intense fear.
According to the National Institute of Mental Health, nearly a third of adolescents have an anxiety disorder, with about 8% suffering from severe impairment that leads to poor performance in school or missing school altogether; avoiding social situations; isolating; and/or using alcohol or drugs to mask the pain. They often feel alone and ashamed, and their anxiety can contribute to other conditions such as depression and eating disorders.
Studies show that during the COVID-19 pandemic, depression and anxiety in kids and teens doubled compared to pre-pandemic levels. One in 4 youth have significantly higher depression symptoms, while 1 in 5 are experiencing clinically elevated anxiety symptoms.
Although the cause of anxiety and panic attacks is varied, it can include a trauma, a divorce or death in the family or a physical illness. Plus, some people may be biologically predisposed to anxiety and panic attacks.
Here are some suggestions on how to help:
Encourage your daughter to speak openly about her feelings. She needs to know that she isn’t at fault when she experiences symptoms of anxiety or panic.
Assure her that, although she may feel she is crazy or is going to die, she is not in any danger.
If she associates a certain place (such as school) with a panic attack, she may start avoiding that situation. Gentle, gradual exposure is essential, since continued avoidance only strengthens the pattern.
News and social media can impact children much more than adults, causing them to feel unsafe in their environment, so it’s wise to monitor what your children are watching on TV and on social media.
Make sure she eats healthy meals, gets enough sleep and exercises. Being physically healthy can lessen the effects of anxiety and panic.
Some other important steps to take include getting an evaluation from a medical professional to rule out any physical ailments that may contribute to anxiety.
The good news is that panic and anxiety disorders are very responsive to treatment, so contact a mental health agency or professional. Tell your daughter that seeing a therapist is a perfectly normal thing to do, and that many kids who experience anxiety are helped through therapy.
During the pandemic, North Shore Child & Family Guidance Center is seeing clients both remotely via telehealth platforms and in person, depending on the clients’ needs. To make an appointment, call 516-626-1971 or email intake@northshorechildguidance.org.
Children of all ages with mental health challenges and learning disabilities can benefit enormously from involvement in the arts. According to Scientific American, creative endeavors stimulate different parts of the brain than other forms of learning, which can create a positive environment for kids who have special considerations to contend with in terms of typical learning structures. When children and teens express themselves through the arts, whether it be painting, acting, music or other avenues, it can help lower stress and anxiety, improve self-esteem, moderate their moods, and create stronger relationships and social skills. In addition, it can have a positive impact on their academic life.
Below, you’ll find some information on how your child or teen can benefit from the arts and how to get them started.
How the Arts are Different
There’s a difference between painting a picture or molding clay and reading textbooks or performing mathematical calculations. According to a report by Americans for the Arts, children exposed to creativeendeavors perform better academically and have more advanced language skills than those who don’t. While children with learning disabilities do require assistive approaches to help them master traditional foundational educational concepts, incorporating the arts provides an environment in which they can feel good about their abilities and have something concrete they have control over. This can be especially helpful for teens, who go through so many changes in these pivotal years and often feel like they can’t control anything in the world around them.
Arts and Crafts at Home
If you have a teen with learning disabilities or mental health issues, ensuring you have plenty of arts and craft supplies at home can help them expand their imaginations with hands-on creative pursuits. You might allow for freeform activities or employ the use of online tutorials to encourage specific forms of artistic activity. Combining both structured and unstructured access to the arts can help your teen follow directions and step-by-step instructions, while still encouraging creativity.
Explore Different Types of Creative Pursuits
Involve your child in deciding what kinds of arts they’re most interested in. According to website Design Swan, there are a range of things you can do at home, including pottery, painting, jewelry making, watercolors and papercrafts. Teens may also be interested in taking classes in such media as oil painting, glasswork or ceramics. Check your local community art centers to learn about beginner classes that are available for young people. You might even consider joining them in the class! Not only can this be a fun bonding experience, but it will also give you greater insight into the way your child participates in a classroom environment and help you identify how you can help them manage their challenges.
The arts offer a great opportunity for teens with disabilities and mental health concerns of any kind find something they’re passionate about, develop a healthy outlet for expression, and even improve their academic performance. It’s a great way for them to develop their emotional health and set a strong foundation for making smart choices now and long into the future.
Bio: Colleen Stewart loves giving her two kids a healthy example to live by. Her passion for community and wellness inspired her and her husband to team up with their neighbors and create a playgroup that allows the adults and their kids to squeeze in a workout a few times a week. She created Playdate Fitness to help inspire other mamas and papas to make their well-being a priority, and set a healthy foundation for their little ones in the process.
By Jessica Grose, published in the New York Times on February 16, 2022
“A mother’s internalized mandate to protect her child does not end when her children are grown”
We have a mainstream directive for raising children in our society: You provide them with support, shelter and care until they’re 18, and then they’re supposed to be, more or less, self-sufficient, launched into the world as adults. This framework leaves out millions of parents whose children struggle with substance abuse or mental illness, who may be providing active care to their adult children for the rest of their lives.
A new book, “Difficult: Mothering Challenging Adult Children through Conflict and Change,” by Judith R. Smith, an associate professor at the Graduate School of Social Service at Fordham, seeks to define and explore this often painful type of parenting. An estimated 8.4 million Americans care for “an adult with an emotional or mental health issue,” according to a 2016 report from the National Alliance for Caregiving, and 45 percent of mental health caregivers are caring for an adult child.
For “Difficult,” Smith writes, she spoke to 50 mothers of adult children who were not fully independent, who had issues from severe mental illness to persistent unemployment. All of these mothers were over 60, and many were also dealing with their own declining physical and emotional health. Smith writes that half the women she spoke to were doing this with incomes under $17,000 a year for a family of two.
“My research revealed that a mother’s internalized mandate to protect her child does not end when her children are grown,” Smith writes, and she outlines the stigma and worry they feel about their children’s problems. She seeks to lessen this stigma for parents, more and more of whom will be in the same situation as her book’s subjects in the coming years, with young adults increasingly reporting mental health issues, particularly during the pandemic, and the opioid crisis continuing to take lives.
There is very little social support for these parents and their children: According to the National Alliance for Caregiving, the majority of adult caregivers have trouble getting services for their loved ones like day programs or peer support, and close to half say they struggle to find treatment for substance abuse. Just as for younger children, mothers are spackling over every gap in the system, sometimes destroying themselves in the process. Sixty-two percent of parents who are caregivers for adult children say their caregiving role has made their own health worse.
I spoke to Smith about how she chose the term “difficult adult children” to refer to this population, what can be done to help caregivers and their children in the near term and why it’s important for all parents to come to terms with their own ambivalence, because it is normal to have mixed feelings about our roles. The following conversation has been edited and condensed.
Jessica Grose: Tell me about the choice to use the term “difficult adult children,” and what it means for the mothers in your book.
Judith Smith: As I was doing my research, one friend said, “No, no, no, you can’t use that word. It’s pejorative.” But as I say in the book, this is how difficult is defined: It’s something hard to do, it’s something hard to manage, and it’s something hard to understand.
Whether the kid had a substance use issue or severe mental illness or was depressed or unemployed and not willing to look for a job, what I heard was the mothers were struggling. It was really difficult for them to figure out what to do, because they didn’t see any choice. They felt committed as mothers to hang in there, but they felt hopeless for their child and they felt hopeless for themselves. Some of them were in real physical danger, living with an adult child who had serious problems.
Jessica Grose: I was so struck by the point that you made about how for mothers of children with mental illness who are in danger, that often their only option is to call the cops. Most parents do not want to call the police on their children. You also talk about the very limited options in the United States if parents are not able to take on the work of housing and protecting their children anymore. What’s the low-hanging fruit of what we can change to help these parents in the near term? I know this is a decades-long, complicated, multipronged problem.
Judith Smith: I think the advocates for parents of adults with severe mental illness are hoping for something they call “housing that heals” — supportive housing, group homes for people with severe mental illness that also have treatment. I think housing has to be a priority. There also need to be more psychiatric beds available for when people need them in the short term. This is a political battle within the advocacy for severe mental illness. In terms of the people who advocate for the rights of the person with mental illness, and the families who would like there to be more options for temporarily taking away the rights of the person and having them be protected and hospitalized when they are really aggressive and a danger to themselves and their families. But it’s a horrendous decision to say, “Right now, my child will have to be homeless.”
Jessica Grose: Reading about mothers in your book grappling with that decision was just awful. And I think part of why it was so awful for them is because of the blame that society tends to place on mothers. You quote the psychologist Stella Chase, who said, “There are very few jobs in which one individual will be blamed for anything that goes wrong, and fewer still in which what can go wrong, and the feeling of being blamed, is so devastating.” Can you tell me a bit more about how that ends up playing out, in terms of the guilt and shame that these mothers feel?
Judith Smith: I think we assume that women should be able to do everything, and we should be able to produce perfect kids. So I think for all parents, when our kids aren’t doing well, it affects our self-esteem. We feel bad and then we experience the conflict of ambivalence. Rozsika Parker wrote a wonderful book, “Torn in Two,” more than 20 years ago. She’s a psychoanalyst. And she really talks about how shameful it is for women to acknowledge their mixed feelings, which we all have.
If you want to take a shower and your kid won’t let you take a shower, you’re angry, but then you feel bad for being angry. And society doesn’t allow women to have mixed feelings. Parker named the conflict of ambivalence as what is keeping mothers imprisoned and so isolated and feeling so bad about themselves — but that in fact, ambivalence is a part of all relationships. That’s a lot of what we do with clients, is allow them to express negative feelings about their parents or about their spouses and be able to live with it without feeling like they’re bad people.
Jessica Grose: I’ve heard most concepts in terms of the caregiving literature, but I hadn’t heard of “chronic sorrow,” before your book, which is something these mothers experience, and which is defined as “the long-term periodic sadness the chronically ill and their caregivers experience in reaction to continual losses.” I would love to hear you talk a little bit more about chronic sorrow — the hopes these parents once had for their kids that are now gone.
Judith Smith: Each mom I talked to experienced it in a different way. One woman has a 37-year-old son who has been home since college, when he had a breakdown. He was in the Harlem Children’s Choir, had a beautiful voice. Everybody liked him in the neighborhood and none of that is there anymore.
Each person talked about what wasn’t. One mom talked about her sadness at the birth of her first grandchild. It should have been the most joyous time in her life. But it made her remember her first birth, which was her son who ended up dying by suicide at 45. She had three other living children, and she felt so bad that she was feeling sorrowful at such a wonderful moment.
But this is what it is. There is a study where they actually, with large data set, proved that you’re only as happy as your least happy child. There are a couple of books that are written about when our kids disappoint us, and the message is: “Move on, let them take care of themselves.” But they’re not talking about this population. These mothers cannot just move on. Programming note: I’m taking some time off. I’ll be back with another newsletter on March 2.
Featuring Dr. Nellie Taylor-Walthrust and the Birth Justice Warriors, a program co-founded by Taylor-Walthrust and Martine Hackett of Hofstra University.
In Nassau County, babies in communities of color are significantly more likely to die during or shortly after birth than in predominantly white communities.”
U.S. Sen Kirsten Gillibrand, a Democrat from New York, last week called on Congress to provide $7 million to fund evidence-based training programs to reduce implicit bias in maternal health, and $25 million to establish a program to deliver integrated health care services to pregnant women and new mothers that will reduce the inordinately large number of maternal deaths among Black non-Hispanic women.
It is an urgent issue, including here in Nassau County, one that the Herald first called on government officials to address in 2019. We are pleased to see that Gillibrand has taken up the cause.
Three years ago, the Herald undertook a year-long series examining racism in Nassau. We led with an exposé on issues of maternal health faced by Black women throughout the county. In particular, we looked at the group Birth Justice Warriors, founded by Hofstra University Professor Dr. Martine Hackett and the Rev. Dr. Nellie Taylor-Walthrust, a pastor and the director of outreach services for the North Shore Child Family Guidance Center, a nonprofit mental health agency with offices in Roslyn Heights, Manhasset and Westbury.
Among the central issues that Birth Justice Warriors is working to address is infant mortality, which is a leading indicator of a community’s well-being, according to the Nassau County Department of Health’s 2016-18 Community Health Assessment and Community Health Improvement Plan. When children are dying in high numbers at birth — the start of life — there are probably myriad other health concerns in a community.
In the majority of white communities across Nassau, the infant mortality rate ranged from 0 to 3 in 1,000 births in 2014-16, according to the state Department of Health. Meanwhile, in most communities of color, the infant mortality rate was three to nine times that.
In its annual rankings of healthiest counties in New York, the Robert Wood Johnson Foundation, working with data from the federal Centers for Disease Control and Prevention, ranked Nassau the second-healthiest of the state’s 62 counties this year. When that data is broken down into individual ZIP codes, however, a disturbing pattern is made clear in communities of color, Hackett said: Babies there are significantly more likely to die during or shortly after birth than in predominantly white communities.
County officials identified nine communities of color and communities with large minority populations — Elmont, Freeport, Glen Cove, Hempstead, Inwood, Long Beach, Roosevelt, Uniondale and Westbury — with measurably greater health concerns than nearby white communities.
Nassau is the 13th-wealthiest county in the U.S., with an average annual household income of around $93,000, according to census data. “The affluence of the county as a whole masks the needs of these severely underserved selected communities,” the county’s report states.
Taken as a whole, the infant mortality rate in these communities is “nearly double that of the rest of the county,” the report continues.
The knee-jerk reaction is to blame the discrepancy on a discrete factor like income level, according to Hackett: Women with fewer financial resources are unable to afford the same level of care that women of greater means can. But statistics tell a more complicated story.
How, for example, does one explain Elmont, a solidly middle-class community of color with an annual average household income of $94,353, above the county average? It has the second-highest infant mortality rate in Nassau.
Access to health care alone “is not sufficient” to explain the disparities in health outcomes, Hackett said. Bias and systemic racism also play their parts, she believes.
Clearly, issues of implicit bias, and at times outright racism, come into play, even in the medical field. It’s time that the federal government study and address them so all of us can better understand the psycho-social complexities of the doctor-patient relationship that can determine maternal health outcomes.
February is Black History Month. Historically, there is a great deal of mistrust in Black communities of the medical field because of past wrongs, not the least of which was the infamous “Tuskegee Study of Untreated Syphilis in the Negro Male” from 1932 to 1972, when Black sharecroppers with the venereal disease were left untreated to see what would happen, even after penicillin, a cure for syphilis, was widely available after 1945.
The only way to build trust in Black communities is to address their issues head-on, with science-based studies and programs, as Gillibrand has proposed. Congress thus should appropriate the funds that the senator seeks.
In this monthly column, therapists from North Shore Child & Family Guidance Center answer your questions on issues related to parenting, mental health and children’s well-being. To submit a question, email communications@northshorechildguidance.org.
Question: My daughter is a mostly happy teen. Like all kids, she gets down sometimes, especially during the pandemic. But what I’ve noticed is that her mood seems to change dramatically in the winter. She becomes lethargic, unmotivated and sad. It’s a very noticeable difference from other times of the year. Is this a common thing with teens? What can I do to help her?
Feeling Blue for My Girl
Dear Feeling Blue: It sounds like your daughter may be one of the six percent of the population who experiences SAD, which stands for seasonal affective disorder. While some level of winter blues isn’t uncommon, for some people, the shorter, darker and colder days that characterize this time of year cause clinical depression.
While SAD typically begins in a person’s early 20s, older children and teens can develop the condition. More than simply the “winter blues,” SAD is characterized by feelings of sadness and hopelessness nearly every day. People with SAD are unable to enjoy the activities that typically make them happy; they have difficulty concentrating and are often tired and/or agitated.
Two chemicals in the brain—melatonin and serotonin—are responsible for regulating energy, sleep cycles and mood. During winter’s darkness, melatonin levels increase, causing sleepiness and fatigue. Serotonin, which is sometimes referred to as the feel-good chemical, is produced in greater amounts with exposure to sunlight, and we naturally get less light in the long, cold days of winter.
Some people suffer from a lesser form of SAD, whose symptoms include low energy, weight gain, craving carbohydrates and social withdrawal.
Some other facts: Females are about four times more likely to develop SAD than their male counterparts. People with a history of depression are more prone to experiencing symptoms of SAD.
Here are some strategies that you can share with your daughter, whether she experiences full-blown SAD or the milder winter blues (and most of these are useful tips for everyone year-round!):
Get as much direct exposure to sunlight as possible.
Since being out in the sun can be difficult this time of year, either due to cold temperatures or long days inside, consider purchasing artificial “sunbox” lights. Their special fluorescent tubes mimic the sun’s beneficial rays (plain lights don’t have the same effect).
Keep or start an exercise routine. If it’s not too cold out and it’s a sunny day, try to walk outside to reap the benefits of being in natural sunshine—but even if you work out indoors, it will have a positive impact on your mood.
Turn up the heat (between 64 and 70 degrees) and drink hot beverages.
Eat healthy foods, with a focus on fruits and vegetables. That’s good advice any time of year, but especially important in winter when your cravings for sugar and carbohydrates tend to increase.
Don’t give in to the urge to isolate. Seeing friends and attending social functions are crucial to putting a damper on the blues.
Keep active by engaging your creative side, whether it be taking up a new hobby or reintroducing a former favorite pastime. Encourage your child to participate in after-school clubs and other activities.
Take up meditation and other mindfulness-based practices. You can find literally thousands of guided meditations on a free app called Insight Timer.
Finally, keep in mind that if your daughter’s depression is impacting her ability to function, it’s important to seek help from a mental health professional—regardless of the season.
During the pandemic, North Shore Child & Family Guidance Center is seeing clients both in person and remotely via telehealth platform. To make an appointment, call (516) 626-1971 or email intake@northshorechildguidance.org.
By Paul Danilack, Published in Anton Media, January 20, 2022
Growing up, Timmy appeared to be a little bit different than other children his age. He would cry often and have frequent temper tantrums. His parents brought him to see an early intervention therapist, and his symptoms lessened for a few years. But in middle school, his frustration returned in the form of anger, both verbal and physical. Typical back talk turned into confrontations. Timmy would throw objects and began to attack his parents. They eventually reached their limit and started giving into his behaviors to stop the fighting.
Timmy’s parents felt alone and helpless. They didn’t know where to turn to get their child the care he so desperately needed until a school guidance counselor suggested they call North Shore Child & Family Guidance Center and ask about the Family Advocate Program.
Through this innovative program, parents who are overwhelmed trying to navigate the maze of services available for their child are paired with one of the Guidance Center’s Family Advocates. These credentialed professionals aren’t therapists; rather, they are parents of their own children with special needs and are trained to educate, teach, guide and empower other parents to better understand their children and their needs.
With an individualized, family-driven approach, the Guidance Center’s Family Advocates meet with the parents to learn about their child’s particular issues. Some children have serious behavioral problems, acting out verbally or even physically. Some refuse to go to school. Some struggle with severe anxiety or depression. Many of the problems children are living with have been exacerbated by the stresses caused by the pandemic.
Family Advocates provide a wide range of information and support, attending evaluations with parents; going to CSE (Committee on Special Education) meetings; helping build skills within the family to manage difficult behaviors; finding residential placement when indicated; and seeking inpatient hospitalization if needed. In addition, while Family Advocates don’t provide therapy, they can help parents and their children access those services.
Family Advocates work with parents and the child’s therapist to help design a plan to modify their youngster’s negative behavior. For example, Family Advocates help parents create behavioral charts to develop a uniform approach of rewards and consequences. These strategies help motivate children to listen more carefully and respond in appropriate ways. Moreover, Family Advocates can act as a bridge to many services, such as the school, individual counseling, case management and more, so everyone involved in the child’s life are on the same page when it comes to addressing his or her needs.
Families with children who have developmental disabilities often feel secluded and without support. The Guidance Center’s Family Advocates are well informed about New York State’s Office for People with Developmental Disabilities as well as the process to become eligible for those services, which include respite counselors, community habilitation workers and housing availabilities, among others.
Another important feature of the Family Advocate Program is a weekly support group (now mostly virtual, though in person once a month), where parents share their challenges and successes, bouncing ideas off each other, talking about what worked and what didn’t, and building a social support network with others who are experiencing similar challenges. They learn that they are not alone, and they develop close, caring relationships with their parent peers.
In summary, Family Advocates work to empower each family with a personalized approach, with recommendations and assistance based on what’s best for each client. They care deeply about every family as demonstrated by their compassion toward and knowledge of what can be a very difficult situation.
There’s no doubt about it: The pandemic changed the workplace forever. Estimates are that in 2021, about a quarter of American employees worked at home at least part of the time. It can be assumed that a moderate to a significant portion of these workers had young children at home.
Creating a balance between remote work and young children can be difficult, especially during the pandemic, but it isn’t impossible.
Here are some suggested strategies that can help you successfully manage working at home with little ones:
Use Freelancers to Lighten Your Workload
A freelance virtual assistant (VA) can help lighten your workload by handling small administrative tasks. For example, you could hire a VA to make phone calls, schedule appointments and handle simple emails. A VA can also format and schedule blog posts and manage some (or all) social media postings. Other duties can be assigned, depending on your industry. In the wake of the pandemic, virtual assistant jobs have been on the rise.
You can find virtual assistant services on job boards, dedicated online platforms and even (sometimes) relevant social media groups. Before hiring anyone, make sure you either read reviews or get references. You’ll also want to weigh out the costs versus how much time you’ll save.
Consider Your Childcare Options
Thanks to the pandemic, many parents now work from home and care for their kids by themselves, but this can be both overwhelming and a productivity killer. Consider reliable childcare options, even if they’re only part-time. For example, you could look to your support system for help. Could one of your parents or siblings sit with the children for a few hours twice a week? Could your spouse take an hour after they get home for the day?
Another option is professional childcare or daycare. Sending your toddler to daycare even two or three days a week for a few hours could help you get a lot more work done. If finances are an issue, look into state assistance. Most states have options to pay a percentage of total childcare costs as long as the facility is eligible.
Work Smarter
Despite your best efforts, your mind can only focus on a task for so long before you begin to lose concentration. Consider using the Pomodoro technique. With this method, you work for 25 minutes and then take a five-minute break. You repeat this four times, and then allow yourself a longer break.
While the actual method states the longer break should be 15 to 20 minutes, parents can alter this technique to fit their lifestyle. For example, you could take a 30-minute or even one-hour break to spend time with your young children. You can schedule these breaks around breakfast, lunch and nap time, or use one of these breaks to take your toddler outside to play for a short period.
Practice Meditation
Meditation can help you feel more in control of your life. It can also help reduce feelings of anxiety, depression and stress. Have your toddler sit and practice meditation with you for five minutes each day, and then take five or 10 minutes for yourself in the evening. Not only will you be practicing self-care, but you’ll also be teaching your toddler an excellent coping technique.
Bio: Colleen Stewart loves giving her two kids a healthy example to live by. Her passion for community and wellness inspired her and her husband to team up with their neighbors and create a playgroup that allows the adults and their kids to squeeze in a workout a few times a week. She created Playdate Fitness to help inspire other mamas and papas to make their well-being a priority, and set a healthy foundation for their little ones in the process.
As we settle into the new year, a look back at 2021 brings up mixed emotions.
What a rollercoaster it was! The biggest news story remained the same as in 2020: the COVID-19 pandemic. While the vaccine brought hopes for a return to more familiar times, the pandemic had other plans, and today, we are in the midst of a surge that brings with it more uncertainty.
Like all of us, kids and teens are emotionally drained from all the ups and downs, but they’ve faced upheaval at a crucial time in their development. The result: In the past 22 months, rates of depression, anxiety and other mental health issues among youth have skyrocketed, and our services have been needed more than ever before.
Despite the unprecedented challenges, the two words that jump to my mind when reflecting on 2021 are these: Gratitude and hope.
North Shore Child & Family Guidance Center is blessed to have an abundance of dedicated supporters like you who answered the call when we requested donations to support our life-saving work. Your generosity made all of us at the Guidance Center grateful.
And knowing we could count on you—and can continue to count on you—filled us with hope as we bring healing to families across Long Island who are struggling to find their way.
Here is just a small sample of what your donations have meant for the children and families of your community:
We gave much-needed bereavement therapy and comfort to children as young as three years old who lost a parent or other loved one to the coronavirus.
Through our Douglas S. Feldman Suicide Prevention Project, we treated young people at high risk for suicidal thinking through multiple weekly sessions of individual, group and family therapy, along with a culturally sensitive treatment plan focused on safety strategies, healthy coping skills and relapse prevention.
As part of our Diane Goldberg Maternal Depression Program, we provided treatment and support for moms experiencing postpartum depression during a time when hospitals prohibited partners from being present at births, and other birth plans were being interrupted by COVID.
These successes are directly attributable to your care and concern for your community. Because of you, the entire staff at the Guidance Center enters 2022 feeling hopeful and deeply grateful.
Wishing you and yours good health,
Kathy Rivera Executive Director/CEO, North Shore Child & Family Guidance Center